

Genetic and Clinical Background:
The clinical outcome of Core Binding Factor Leukemia (CBFL) seems influenced by the mutational status of KIT. In fact, several retrospective studies, in addition to our own, as well as a systematic review, indicate that KIT mutations have a negative prognostic impact in AML with t(8;21) or, to a lesser extent, with inv(16)/t(16;16).
In addition, gene expression studies found KIT to be highly expressed in CBFL regardless of its mutational status. Furthermore, recent studies have identified novel recurrent somatic mutations co-occurring with KITmut.
In-vitro studies revealed that Midostaurin (Mido) is effective in inhibiting both wild type (WT) and a range of KIT mutants. In addition, it is proven to be effective in KIT-positive malignancies such as Aggressive Systemic Mastocytosis (ASM), Mast Cell Leukemia (MCL), and SM with Associated Hematological Neoplasm (SM-AHN).
With this background, we designed a Phase II trial to evaluate the safety and efficacy of Mido in association with Intensive Chemotherapy (IC), in CBFL regardless of KIT mutational status.
Methods:
The inclusion criteria were the following: age 18 to 60 years, diagnosis of de-novo CBFL, adequate organ function, signed informed consent. The exclusion criteria were: central nervous system involvement, uncontrolled infections, other active malignancies, a Qtc value greater than 470 ms (according to Bazett formula) at the electrocardiogram, significant uncontrolled or active cardiovascular diseases.
Patients received standard induction therapy with an anthracycline containing regimen ("7+3"-like) + Mido, three cycles of post-remission consolidation chemotherapy with high-dose cytarabine + Mido, and 12 months of Mido as Maintenance.
The Mido dosage was: 50 mg orally twice a day, on days 8-21, in association with IC, and 50 mg orally twice a day as single agent maintenance.
In order to attain a reduction in 2 years Relapse Incidence (RI), from the historical value of 48% to 28% (Primary Objective of the Study), we plan to enrol 39 patients (power 82%, alpha error 4,6%). At diagnosis all patients were studied by a comprehensive NGS panel targeting 40 DNA genes and 29 RNA fusion driver genes. MRD status was assessed by qPCR and high-resolution multicolor flow cytometry at established check-points during consolidation and maintenance therapy.
Results:
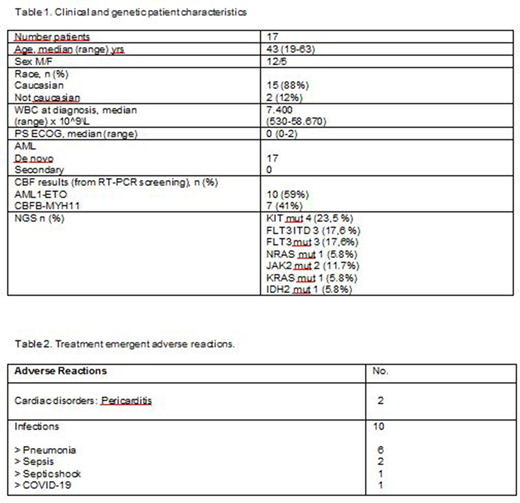
17 patients were enrolled between December 2018 to April 2020 (table1). Overall, the CR rate was 94.2%. At a median follow-up of 9 months (range 3-19 months), we recorded a RI of 12.5%, an OS of 93.7%, and a DFS of 81.2%. 16 patients continue on study and 14 patients are in 1st CR, MRD-negative by flow cytometry and qPCR.
Six patients (35.2 %) experienced 12 Treatment Emergent Adverse Event (TEAE), 10 out of whom were infections, with grade 3-4 neutropenia (Table 2). We only recorded one death from SARS-Cov2 infection (Interstitial Pneumonia) in a patient in MRD-negative complete remission. There were no treatment-related deaths.
Conclusion:
In patients with CBFL, the regimen consisting of intensive chemotherapy and consolidation chemotherapy in association with Mido, followed by Mido maintenance, had an acceptable safety profile and excellent response rates with a significant proportion of patients in MRD-negative complete remission. Trial is continuing to accrue (EudraCT Number 2017-002094-18; ClinicalTrials ID: NCT 03686345). This work was supported by a grant from Fondazione Regionale per la Ricerca Biomedica (FRRB 2015).
Krampera:Janssen: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Todisco:Jannsen, Abbvie, Jazz: Membership on an entity's Board of Directors or advisory committees. Veronese:Novartis: Other: Travel Expenses; Bayer: Honoraria; AstraZeneca: Other: Travel Expenses; Janssen Cilag: Honoraria.
Midostaurin for treatment of Core Binding Factor Leukemia. The drug has been used as KIT inhibitor.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal